Community-Centric Research on Aging Adults
 Community-Centric Research on Aging Adults and Access to Healthcare in the Upper Valley of New Hampshire
Community-Centric Research on Aging Adults and Access to Healthcare in the Upper Valley of New Hampshire
We are three Dartmouth students in a spring 2021 class about rural sociology, and we have been conducting research by assessing both data and primary source interviews with community members over the past two months. We are taking a social impact practicum (SIP) class which means that while we study a topic in class, we are simultaneously given the opportunity to work with a local organization or group to gain some firsthand experience in the field. This also allows us to gain a broader perspective on the greater Upper Valley community, its strengths challenges, and idiosyncrasies. The three of us have been privileged to work with the Public Health Council of the Upper Valley (PHC) researching access to healthcare and other resources for the local aging community. We would like to thank the PHC, the Center for Aging Resources at DHMC and all the people who participated in our focus groups and individual interviews for being open, honest, and helpful to us throughout this project. — Hannah Lang, Kate Miller & Katherine Ogden
Town-Specific Findings:
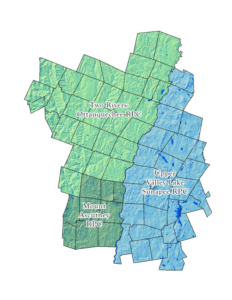
The Upper Valley of New Hampshire consists of 12 towns nestled into the Connecticut river valley. Of the 12 towns in the area, Lebanon has the largest population of people over the age of 65 and has the most centralized senior living establishments. Focus group participants generally spoke very highly of the access to healthcare and other resources in Lebanon. Grafton and Canaan have higher rates of poverty in their elder populations, making these towns potentially ripe for specific affordable or free resources and interventions. Hanover and Lyme on the other hand have wealthier populations but these towns still struggle with social isolation, fall risk and ability to accomplish upkeep tasks around the home. Dorchester has the highest rate of annual ER visits per 1000 people over age 65. While this statistic could be slightly skewed by low population it is still indicative of significant need in the area.
We developed a Data Brief to summarize our findings, which you can download from this post.
Strength of Senior Centers
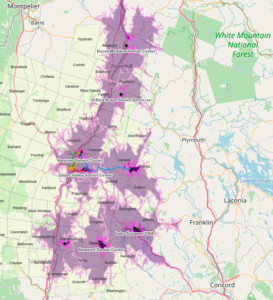
This map shows Upper Valley towns in New Hampshire. The light purple area indicates areas within a 20 minute drive of the senior center, the dark purple area indicates areas within a 5 minute drive. The Advance Transit bus route is also included on the map. Most areas have a senior center within a relatively short distance, though they may be inaccessible to seniors who are no longer able to drive and do not have a reliable source of transportation. For a live map, see: https://arcg.is/1iCanX
In terms of both culture and community the Upper Valley has some very notable strengths. In our focus groups we found many people feel good about reaching out to neighbors, friends, and family members for help with tasks around the home. We also learned that the Upper Valley has a very strong network of senior centers. Lebanon, specifically, has a senior center that many of the focus group participants both loved and, in many cases, relied on. Senior centers are particularly impactful for providing social spaces for this population as well as medical, nutrition and transportation recourses.
Community Nursing Resources
Many towns in the area also have access to community nurses and community health centers. These are very important resources for people to use while aging in place. Community nurses are able to help their clients without being beholden to insurance regulations because they are funded through either grants, charity or town finances.
Recommendations
One area for intervention in the Upper Valley is providing senior centers in more rural towns or providing access to existing centers in neighboring areas. These centers are hubs of social connection while acting as a safety net to help head off health issues before they become emergencies.
Similarly, many of the towns have access to community nurses but some do not have this recourse. In discussion with a community nurse in Lebanon, it also became apparent that she and her colleagues are both overworked and not always experts in the care they are providing. One place where this problem could be combatted would be access to more mental/cognitive health recourses so that this burden does not fall on community nurses who are untrained in the area. More access to social workers, mental health workers and care coordinators would be very effective for helping to streamline care for individuals who prefer to age in place.
When discussing interventions and increasing accessibility, everything generally comes down to increased funding. One way to create access to more funding for aging resources is just to increase cultural awareness and understanding of the aging population. With more state and federal level funding, it would be easier to make sure that more introverted or isolated seniors do not fall through the cracks. At present the communities are already taxed so it becomes difficult to do the work to extend and advertise existing resources to those who are not actively seeking them out.
Many focus group participants brought up the fact that while they are aware of resources available to them, their less computer savvy or more socially isolated peers could find simply knowing what resources exist to be difficult. Increasing awareness of challenges facing the aging population is an efficient way to help gain funding while also helping to advertise what resources are already organized and functioning.
*One thing to note is that our focus groups were recruited through the Center for Aging Resources. This means those who participated are already engaged within their communities and are outgoing enough to choose to participate in a discussion without any incentive.
Editors Note:
This report focuses on New Hampshire towns in the PHC region because the primary data resource is available only for New Hampshire towns. Comparable data was not readily available for our Vermont towns. Given our experience working in the Upper Valley, we believe the findings that describe the disparities, strengths and resources for older adults are generalizable to many of our Vermont towns as well.